Update on transcutaneous microneedles for antiretroviral drug delivery
pipeline report on novel CAB formulations
Speaker: Ryan Donnelly, Queen’s University Belfast

Microneedles (MNs) deposit nano-formulated drugs in viable skin layers for sustained release (weeks to months) and absorption into the rich dermal microcirculation.
- Desirable characteristics.
- Avoid injections (enhance patient and HCW safety and patient acceptability); Support sustained drug delivery; Co-administration of several drugs is possible (suitable for HIV treatment and PrEP); and Self-application by patients is possible (no clinic visit).
- Review of formulation and application of LA ARV microarray patches.
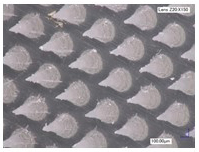
- Load micron- and nano-particulate drugs at high concentration into aqueous gels; Cast into a mold and dry; Add adhesive and occlusive backing layer to form microarray patch (MAP).
- Ideally baseplate should readily detach when MNs dissolve into skin for short wear time.
Pre-clinical PK studies of dissolving MNs for LA delivery of RPV, Etravine, CAB, and Bictegravir in rats.
- Sustained release from 28 to 56 days can be achieved, depending on the actual drug.
- CAB MAP plasma levels were lower than CAB LA IM or ID, but were above therapeutic targets, regardless of CAB formulation (free acid or sodium salt of CAB).
- It is challenging to extrapolate from small animals to humans, particularly with the flip-flop PK exhibited by most LA formulations.
PBPK modeling of MAP delivery of CAB and RPV for HIV treatment in children based on animal data and ex vivo skin deposition in collaboration with PATH and Pharmetheus.
- The estimated patch size required to achieve therapeutic targets increases as the weight band increases, limiting the dosing interval in larger patients.
- Q1M application may be possible in the smallest children (14cm2 patch estimated for CAB and 17cm2 for RPV in the 3 to <6kg weight band), but not for patients ≥35 kg (119 cm2 patch for CAB and 252 cm2 for RPV).
- Q1W application may be possible for larger children and adults (estimated 30 cm2 patch for CAB and RPV in patients ≥35kg).
- ARVs with higher potency may enable Q1M dosing in larger patients – two high potency HIV drugs have been recently evaluated.
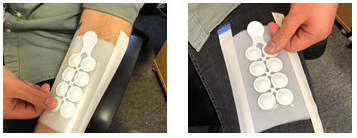
To apply large patches, a series of smaller patches are mounted on a common backing. We evaluated the usability of placebo MAP prototypes with a feedback indicator for delivery of HIV drugs.
- PATH developed a “bubble-type” removable applicator for the MAP prototype (8 large patches [2.5cm2] with 110 MNs each) – when the domes are depressed (visual and tactile feedback), the force should be sufficient to insert the MNs for drug delivery.
- Naïve MAP users (healthy volunteers) actuated the MAP prototype into simulated skin (8-layer parafilm) applied to the arm and thigh by pressing on the domes.
- Optical coherence tomography imaging – 50% of the length of the pyramidal tip was inserted into the simulated skin and no variation based on location, gender, BMI, or age.
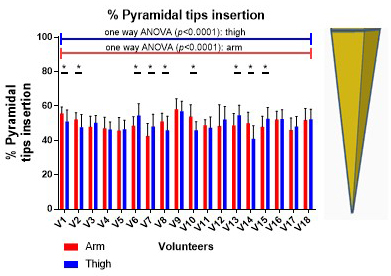
- Users reported easy application and a high confidence level regarding successful insertion.
- Optical coherence tomography imaging – 50% of the length of the pyramidal tip was inserted into the simulated skin and no variation based on location, gender, BMI, or age.
- Implications.
- For larger patches, this removable applicator system can be used to guarantee insertion in every person every time.
- All drugs will need to be in that 50% of the tip length to ensure drug delivery.
- For the two highly potent HIV drugs recently evaluated, this prototype should be sufficient for weekly and potentially monthly application for all patients, not just small children.
Considerations for next steps
- Drugs studied to date are only suitable for weekly patch application in adults.
- PBPK modelling suggests monthly application in smaller children or weekly application in older children is feasible.
- Work with more potent drugs to enable longer duration of action or smaller patches than previous systems is promising.
- Macaque studies, clinical trials, and scalable manufacture.